It took some convincing, on my behalf as J' wanted to put it all behind her; to forget all about it completely, whereas I did not. I did quite a lot of soul searching, as I knew that J' continued to display stress when talking about events that had occurred and I did not want to coerce her into anything. It was painful for me too, but I felt it imperative at least to garner some information, so as to guide any action in the future. So the first step was taken; that of requesting all the notes about her Hospital treatment.
What may seem a simple request, turned out to be more difficult than anticipated and I sought the help of the Patient Advocacy Service to assist me in this. I was not confident that they would be of any use but was pleasantly surprised by the case officer appointed, Andrew (not his real name, which I never knew) whose knowledge and understanding was of great help. So we submitted a request for the medical notes and sat back and waited, and waited. Well it took an age, cost some £50 and came in instalments. And of course you have no proof that what you receive is comprehensive, because you do not know what may have been omitted. Some two months later we actually had them all and I commenced the task of review.

My review of the various tests conducted proved to be the most illuminating element of J' treatment and the memory I had of the Paramedics question, about controlling her Diabetes soon became understood. Her preop' blood glucose was 19.50 mmol/L ! That is severe, uncontrolled hyperglycemia, a situation that could only indicate Type 11 Diabetes. In addition she had been given a 'bolus' of several antibiotics including several penicillin's. She has a well documented adverse reaction to this type of antibiotic, which was advised to the Hospital on admission and it was clearly stated on the notes. There was also strangely, a copy of an ECG trace together with a chest X-ray copy (on disc). These were 'ghosts', because no such procedures were undertaken, and let's face it it would be extremely difficult to 'sneak' an ECG onto a patient, with ten electrodes having to be placed onto various parts of the body and the machine, being wheeled into the cubicle, especially as I was there too. Bizarre is the only word I can use for this.

I had already completed some research into Diabetes prior to the GP visit as the only thing that I could recall from College was that the 'Islets of Langerhans' become non-functional and thus produce little to no insulin. J' also had more practical experience than I, as her father had Non Insulin Dependent Diabetes Mellitus (NIDDM) for a large part of his life. But his condition was treated with diet and exercise. That frankly was my take as well because that had been the protocol for most, thirty or more years ago. What had changed it seemed, was the fear of fat and meats, as the diet route dictated that little to no carbohydrate be consumed. As all carbohydrates convert to glucose in the digestive system somewhat rapidly, it also made biological sense to shun them. What had changed then since my studies in the 1960's? Well quite a lot it seemed.
'Big Pharma' in it's ceaseless pursuit of money had become all powerful along with Diabetes UK, an alleged patient advocacy organisation, and their dominance of the treatment paradigm now in place dictated that Diabetics take a cocktail of drugs including it seems Insulin. Insulin Dependent, Non Insulin Dependent Diabetics? Well that seemed somewhat nonsensical. More research was obviously needed and urgently, but we did concentrate our efforts, (for by this time J' was 'onside' about this, if little else), on reducing carbohydrates with a view to elimination.

And so the Complaint System rumbled forward, until we at last had a meeting. I have written about this in detail a while ago and do not propose to go over it again. Suffice to say we were both devastated by the outcome and resolved to pursue things further, but frankly the ground rules kept moving throughout the procedure making it difficult to find our way. The Brown Government, overseen by that most useless of all Health Secretaries, Andy Burnham decided that a change was needed halfway through our complaint, and we were now left with no choice than to complain that we thought we had been dealt with unfairly, and that the 'Local Resolution' system should review the case once more. The response to this was a refusal, leaving the 'last hope', a referral to Parliamentary and Health Service Ombudsman as our final port of call. But at this stage we decided to concentrate on J's various problems and look for as many solutions as we could.
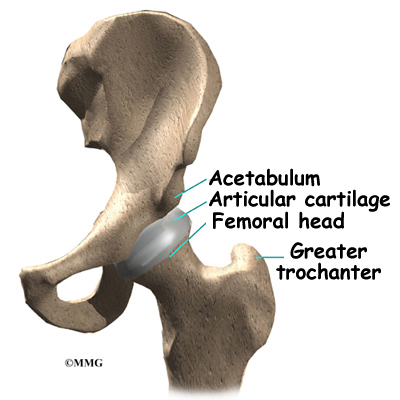
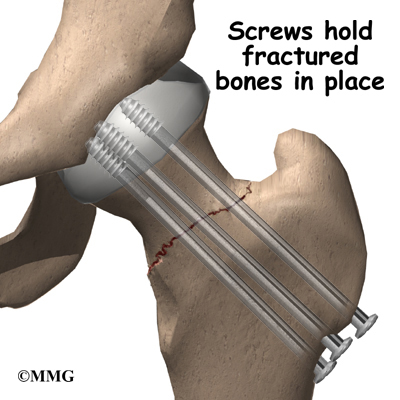
These were; the need to restore her mobility as much as reasonably practicable with the poor prosthesis she had been given.
To control her Diabetes and achieve normoglycemia as much as possible with the minimum of side effects.
And to investigate the pronouncement about her having osteoporosis we found in the notes.
She had a pronounced limp, termed Trendelenburg's Sign, which was placing some strain on her left leg. We needed some physiotherapy intervention for this and, luckily the PCT in the area had a a policy of self-referral, so we did not have to see the GP for this. Using a bit of 'leverage' in my circle of friends, I was able to get her an appointment quickly and we got one of the best in the area. He agreed that J' needed help and devised a work plan that involved resistance exercises that I had to help with, that rebuilt the muscles damaged by the operation. It was hard for her and sometimes painful to see, and often I felt terrible for driving her efforts. But after three long months, it bore fruit and the limp was gone. It also helped with her Diabetes by gist of the exercise needed which reduces insulin resistance in the muscles that helps to lower blood glucose.
Her Diabetes gradually came under control with a low carbohydrate diet, regular exercise with walking and an exercise bicycle, together with a few carefully targeted supplements. Her Hba1c reduced from 8.5 to 6.5 in three months, she lost some weight and the youthfulness she formerly displayed, gradually returned. There was a lot more to achieve as yet, but the walks along the canals helped to keep us both reasonably fit and sane. J' had gone from a vibrant, youthful woman, holding down a well paid job to a partially disabled Diabetic with alleged 'brittle' bones, needing help with at least some aspects of life. She had to have an automatic car, help with getting in and out of bath and could only work part-time.
No one person or organisation was responsible for the accident or the Diabetes, but what the Trust did was to ignore many obvious and relatively simple measures that prejudiced her recovery, her future, her very life even at one point, without any sense of responsibility for their actions and lack of them. No sense of danger in their lax and supine protocols; no remorse, no empathy, but above all no candour and no justice. I had lost my innocence about 'our' NHS, an organisation I had championed in the past, even been grateful to for saving the lives of two of my children. Yet now, after the injection of extra billions in funding, it was actually worse than when it was a service for the poor 'proles' back in 1948. It was devoid of humanity, and the primary tenet governing all that medicine stands for, 'do no harm', because it was doing great harm and 'selling' it as care. It had made an enemy of me and I was to learn in the coming months, many others too. I was no longer 'Winston Smith' and I no longer loved Big Brother.
This saga continues shortly, after I catch my literary breath.